
Cataract Surgery & Lens Implants
INTRODUCTION
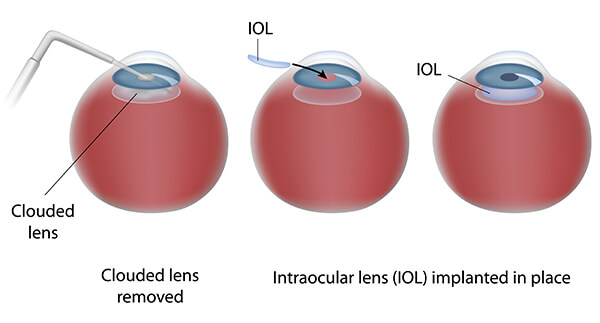
Cataracts interfere with sight because light can no longer pass through. To let light back into the eye, Dr. Seibel performs cataract surgery by removing the cloudy lens. That lens is then replaced with a tiny implantable medical device called an intraocular lens, often referred to as an implant or IOL.
HOW IT WORKS
KINDS OF LENSES
Before intraocular lenses were invented, doctors could only prescribe eyeglasses or contact lenses after cataract surgery. Usually, the eyeglasses had to be extremely thick in order to match the strength of the eye’s natural lens. Along with being rather unattractive, these thick lenses distort the field of vision, resulting in unsatisfactory results. Contact lenses for this purpose were also very thick and often difficult and impractical to use. Intraocular lenses were invented to solve these problems.
About 2 million people per year in the United States have cataract surgery, and almost all of them receive an intraocular lens. There are many different kinds of intraocular lenses for specialized purposes. Your doctor can decide which lens is right for you only after a careful examination of your eye.
IOLs come in two main groups: non-foldable and foldable.
NON-FOLDABLE:
In years past, implants have been made of solid pieces of plastic called PMMA. The cataract incision had to be at least as big as the implant’s optic lens as it is not foldable, or flexible. The common size for these rigid lenses is around 5.5 to 6.0 mm (note this central optic lens is suspended in its position by arms called haptics, which give the implant an overall diameter of 12 to 14mm). A cataract incision of this size usually requires stitches to obtain a watertight seal, and these stitches prolong the healing period
FOLDABLE:
Over the past several years, foldable implants have gained popularity as they can be placed into the eye through a much smaller incision. These implants have flexible optic lenses made of acrylic or solid silicone. They can be placed into the eye through a self-sealing incision as small as 1/8th of an inch. Sutures are not usually required due to the small size of the incision and its self-sealing design. These small foldable implants also enable the surgeon to perform topical cataract surgery, eliminating the need for needle injections and eye patches.
Since the foldable implant enables the surgeon to use a very small incision, these small incisions do not induce significant changes in the patient’s astigmatism, thus enabling predictable results. With predictable outcomes, the surgeon can consider special corneal incisions, called limbal relaxing incisions, to reduce significant pre-existing astigmatism.
These astigmatic corrections are not included in standard medically indicated cataract surgery, but can be optionally done at the time of surgery and can often enable patients with significant astigmatism to enjoy an astigmatic reduction after cataract surgery (not all patients benefit by astigmatic incisions).
STANDARD VS OPTIONAL REFRACTIVE LENS IMPLANTS:
Standard IOL: In medically indicated cataract surgery that is usually covered by insurance, the cloudy lens of the eye (the cataract) prevents light from effectively getting into the eye even when using correction like glasses or contact lenses. The standard lens implant is clear and designed to replace the cloudy lens (cataract) so that glasses or contacts can be effective again as they were before the cataract formed. While the strength of the glasses correction is often reduced overall with standard lenses, it is assumed that patients will continue to need glasses for their best vision for most tasks both near (computer and reading) as well as far (driving and TV). These implants are fixed focus, or monofocal, and as such are usually set so that distance vision is less blurred than near vision; in other words, a patient would be more dependent on reading glasses than distance glasses although they might still need or want both.
Toric IOL: These optional lenses go beyond the medical correction of cataracts by reducing a patient’s need for glasses after surgery. Monofocal Toric IOLs allow good uncorrected vision at a given distance; usually they are set for distance vision to make it likely to pass a driver’s test or see TV without glasses although near glasses would be expected for computer and reading. However, with astigmatism reduced, often simple Over-The-Counter reading glasses can be used for these near tasks. Sometimes patients may have used mono vision with contact lenses, in which one eye is set for distance vision and one eye is set for near; in these cases Toric IOLs can be calibrated in a similar fashion. There is little downside risk to these Toric IOLs when used properly, although a very small percentage of patients may experience a shift in lens position that may benefit from a repositioning in the weeks following the initial surgery.
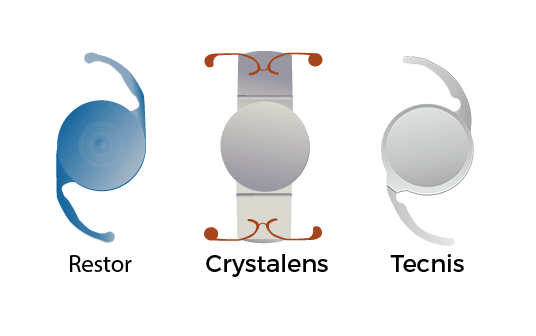
Presbyopia-Correcting IOL: These optional lenses are designed to reduce glasses dependence for both near and far vision. For example, the Technis Multifocal splits light into two focal lengths, for both near and far vision. Patients with this lens typically find greatly reduced or even eliminated need for glasses following surgery. As compared to a monofocal lens (either standard or Toric), a multifocal IOL patient is more likely to notice haloes around points of light, typically headlights or streetlights at night. Fortunately, the majority of these patients (95%) rate the haloes as either mild or moderate, and most of these patients tend to notice the haloes less during the weeks and months following implantation.
Another Presbyopia-Correcting lens option is the pseudoaccomodative Crystalens, which typically has no more glare and halo than a standard monofocal lens (very low); however, the near vision without glasses is typically not as good as with a multifocal, and typically patients require low power reading glasses. The advantage of a Crystalens over a monofocal lens is a greater likelihood of better intermediate vision in addition to distance vision, such as the 3 to 5 foot range where we step on stairs or a curb, or hit a tennis or golf ball; the disadvantage of a Crystalens is that a few patients (about 15% in Dr Seibel’s experience) do not get the additional intermediate vision, and a slightly higher percentage of Crystalens patients (about 2% vs 1% for standard/monofocal/multifocal IOLs) experience lens movement after surgery that can require another surgery for repositioning or replacement.
Another type of Presbyopia-Correcting IOL is the Extended Depth of Focus (EDOF) lens like the Symfony. Like a Crystalens, it is designed to give good distance to intermediate vision, with perhaps a better chance of achieving intermediate vision and potentially at a closer distance of around 2 feet away; patients often still benefit from weak reading and sometimes computer glasses. It has better stability than a Crystalens (around 1% post-op displacement instead of 2%) but it has more glare than a Crystalens, similar to a Multifocal and potentially more noticeable in that it tends to have a spider web or stardust appearance as compared to the more regular round halo or glow of a multifocal. As with the multifocal; patients notice the glare but the majority rate it as mild to moderate and most notice improvement over time.
SURGICAL PROCEDURE
Intraocular lenses are usually implanted during cataract surgery, which is usually performed with local anesthesia. That is, the patient is awake but does not feel the procedure. Under rare circumstances, Dr. Seibel will use general anesthesia, which puts the patient to sleep.
Dr. Seibel makes a very small opening in the front of the eye so the cloudy lens can be removed. There are two ways to remove the lens. One way is to remove it whole, a method progressively less practiced today, and the other is to use a special instrument to dissolve the lens and then suction it out.
Most cataract surgery is done with an instrument that dissolves the lens with ultrasound in a process called phacoemulsification. Be sure to read our Cataract Surgery section for a more in-depth description of this process!
After the natural lens has been removed, the intraocular lens is placed into the eye. Usually, the intraocular lens goes where the natural lens had been. This area of the eye is called the posterior chamber. Sometimes, however, that might not be the best place, so some lenses are designed to be placed in the anterior chamber, the area in front of the colored iris of the eye. The patient is usually ready to go home about an hour after surgery.
For more detailed information, see: Cataract Surgery.
RESULTS
The vast majority of the people, who have cataracts removed, experience higher quality vision after surgery than they had before. An important part of successful cataract surgery with an intraocular lens implant is following your post-operative instructions. Eye drops are prescribed after surgery to help the eye heal better and to prevent infection.
WILL I NEED TO WEAR EYEGLASSES OR CONTACT LENSES AFTERWARDS?
Years ago, before implants were used, patients had to wear very strong glasses or even contact lenses after cataract surgery. This is because the eye was left without any lens and all of the focusing had to be done with the glasses or contacts. Without these visual aides, the patient would have been legally blind.
Today, most intraocular lenses are chosen to focus for distance vision, although the choice is really up to the patient and surgeon to decide. However, until accommodating lenses have technologically evolved enough to pass FDA requirements, IOLs only allow you to focus clearly at a single distance.
Distance vision is usually anything farther than 3 or 4 feet away from the eye. If the lens is focusing at distance, eyeglasses will be needed to see clearly close-up. Many people who have cataract surgery are already used to wearing bifocals, so they are familiar with this type of vision.
Although the implant fitted for distance vision often allows patients to pass a driving test without glasses, many patients may achieve even sharper distance vision with glasses; the choice whether and when to wear a distance prescription is up to each patient.